- Visibility 234 Views
- Downloads 41 Downloads
- Permissions
- DOI 10.18231/j.ijced.2021.052
-
CrossMark

An unusual case report of nevoid hyperkeratosis of areola
- Author Details:
-
 Raajitha N S S Penugonda *
Raajitha N S S Penugonda *
-
P Ramanamurty
-
P.V. Krishna Rao
-
R Roja
Abstract
Nevoid hyperkeratosis of the nipple and/or areola (NHNA) is a rare and benign condition first described by Tauber in 1923. NHNA mostly reported in female patients of child bearing age affecting both the nipples. The aetiology is not well defined and similarly the treatment is empirical. Usually the patient seeks treatment for the cosmetic appearance. Here we report a case of 17-year-old male presented with hyperpigmented to skin coloured verrucous plaques on either side of the right nipple which are asymptomatic and gradually increasing in size since six years. The histopathological features are consistent with nevoid hyperplasia of areola. Till now NHNA has not been reported in young males hence, we report a case of Nevoid hyperkeratosis of the areola in a young male.
Introduction
Tauber in 1923. NHNA mostly reported in female patients of child bearing age affecting both the nipples and areola.[1], [2], [3], [4] Conditions such as Paget’s disease, basal cell carcinoma, seborrheic keratosis and frictional hyperkeratosis should be considered under differential diagnosis.[5] The etiology is not well defined and similarly the treatment is empirical. Usually the patient seeks treatment for the cosmetic appearance.
Case Report
A 17-year-old male presented to our department with two irregular skin colored to hyperpigmented asymptomatic lesions over the right areola of 5 years duration [[Figure 1]]. They started as small mustard size lesions during puberty (at the age of 12 years) and gradually increased in size and number to attain the present size. No history of itching, pain and bloody discharge. No history of any ulceration. No history of any hormone replacement therapy.No other systemic complaints. Not known atopic and no family history of atopy. No similar complaints in other family members.
On examination, two skin coloured to hyperpigmented verrucous plaques on either side of the right nipple. One on the inferolateral aspect of areola measuring 2 x 2.5cm in size and other lesion on the inferomedial aspect of areola measuring 1.5 x 1 cm in size. Few scattered lesions present adjacent to the inferomedial lesion. No erythema, induration, erosion and discharge. No lymphadenopathy. No similar lesions elsewhere in the body. No warts, ichthyosis and acanthosis nigricans.

Routine laboratory tests were within normal limits.
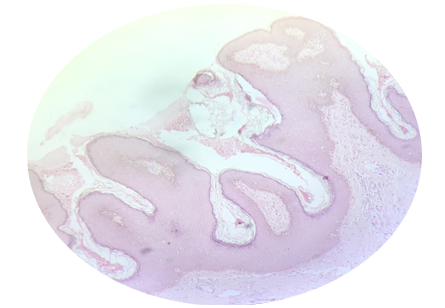
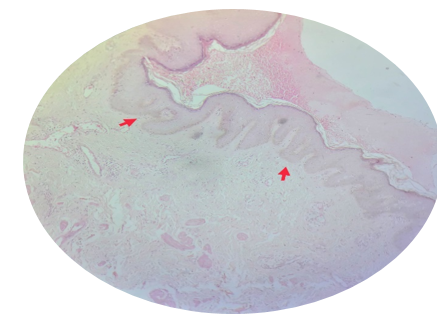
Histopathology sections show papillomatous hyperkeratotic surface with multiple clusters of dilated vessels, downward filiform rete ridges anastomosing to each other with mild lymphocytic infiltration within the dermis. We came to the final diagnosis of NHNA [[Figure 2], [Figure 3]]
She was reassured about the benign nature of the disease and was advice to use keratolytics and steroids with no cosmetic improvement, then complete excision was done, and the patient was followed for 1 year without any recurrences.
Discussion
NHNA is a rare, benign disease mostly seen in females of child bearing age.[1], [3], [4] It is characterized by brown and verrucous thickening of the nipple and/or areola unilaterally or bilaterally. Rarely, hyperkeratotic patches may extend beyond the areolar region. Its etiology remains poorly understood. Few cases were reported - drug-induced, estrogens (for prostatic cancer), spironolactone, and vemurafenib (anti-cancer medication). NHNA occurrence and aggravation around puberty and pregnancy support the theory that NHNA might be a hormonal hyperkeratosis.[6], [7]
Levy-Frenckel in the year 1938 classified NHNA into 3 types [1]
Type 1: Associated with epidermal nevus.
Type 2: Associated with various dermatoses such as acanthosis nigricans, Darier's disease, chronic eczema, cutaneous T-cell lymphoma.
Type 3: Isolated form with an unknown etiology
Recently it is classified into [2]
Primary or idiopathic type.
Secondary type, associated with another skin condition-epidermal naevus, warty tumor, ichthyosis, chronic eczema, Darier disease, acanthosis nigricans, reticulate and confluent papillomatosis, cutaneous T cell lymphoma.
There is no guidelines for treatment, but using Topical agents like Keratolytics, topical Steroids,retinoic acid, calcipotriol and Ablative modalities like cryotherapy, carbon dioxide laser and surgical options like shave excision - curettage, areola removal followed by reconstruction using a skin graft, tangential excision using radiofrequency surgical device can be done.[4]
In conclusion, we report a rare case report of NHNA and its histopathology in young male.
Conflict of Interest
The authors declare that there are no conflicts of interest in this paper.
Source of Funding
None.
References
- Shastry V, Betkerur J, Kushalappa P. Unilateral nevoid hyperkeratosis of the nipple: A report of two cases. Indian J Dermatol Venereol Leprol. 2006;72(4):303-5. [Google Scholar] [Crossref]
- Mehanna A, Malak JA, Kibbi A. Hyperkeratosis of the Nipple and Areola: Report of 3 Cases. Arch Dermatol. 2001;137(10):1327-8. [Google Scholar] [Crossref]
- Ghanadan A, Balighi K, Khezri S, Kamyabhesari K. Nevoid Hyperkeratosis of the Nipple and/or Areola: Treatment with Topical Steroid. Indian J Dermatol. 2013;58(5). [Google Scholar] [Crossref]
- Riley CA, Badri T, Hafsi W. Hyperkeratosis of the Nipple and Areola. [Updated 2020 Sep 15]. In: StatPearls [Internet]. . 2020. [Google Scholar]
- Okan G, Baykal C. Nevoid hyperkeratosis of the nipple and areola: treatment with topical retinoic acid. J Eur Acad Dermatol Venereol. 1999;13(3):218-20. [Google Scholar]
- Félix L, Teja BDL, Guevara C. Nevoid Hyperkeratosis of the Areola and Nipple: A Case Report. Dermatología Cosmética, Médica y Quirúrgica. 2020;18(4):326-30. [Google Scholar]
- Dabas G, Guliani A, Vinay K, Radotra BD. Nevoid hyperkeratosis of male breast: Successful treatment with minocycline. Dermatol Ther. 2019;32(5). [Google Scholar] [Crossref]